Introduction
1.1 Background
Malaria is one of the most devastating infectious diseases worldwide with 241 million (M) cases and 627000 deaths in 2020 (World Health Organization [WHO], 2021). Sudan represents the country most affected with high incidence of malaria in the WHO Eastern Mediterranean Region (EMRO) by contributing estimated 56% cases within the EMRO region (Elagali et al., 2022). This disproportionate burden reflects a confluence of ecological, climatic, socioeconomic and political factors that render Sudan uniquely challenging for the control of malaria.
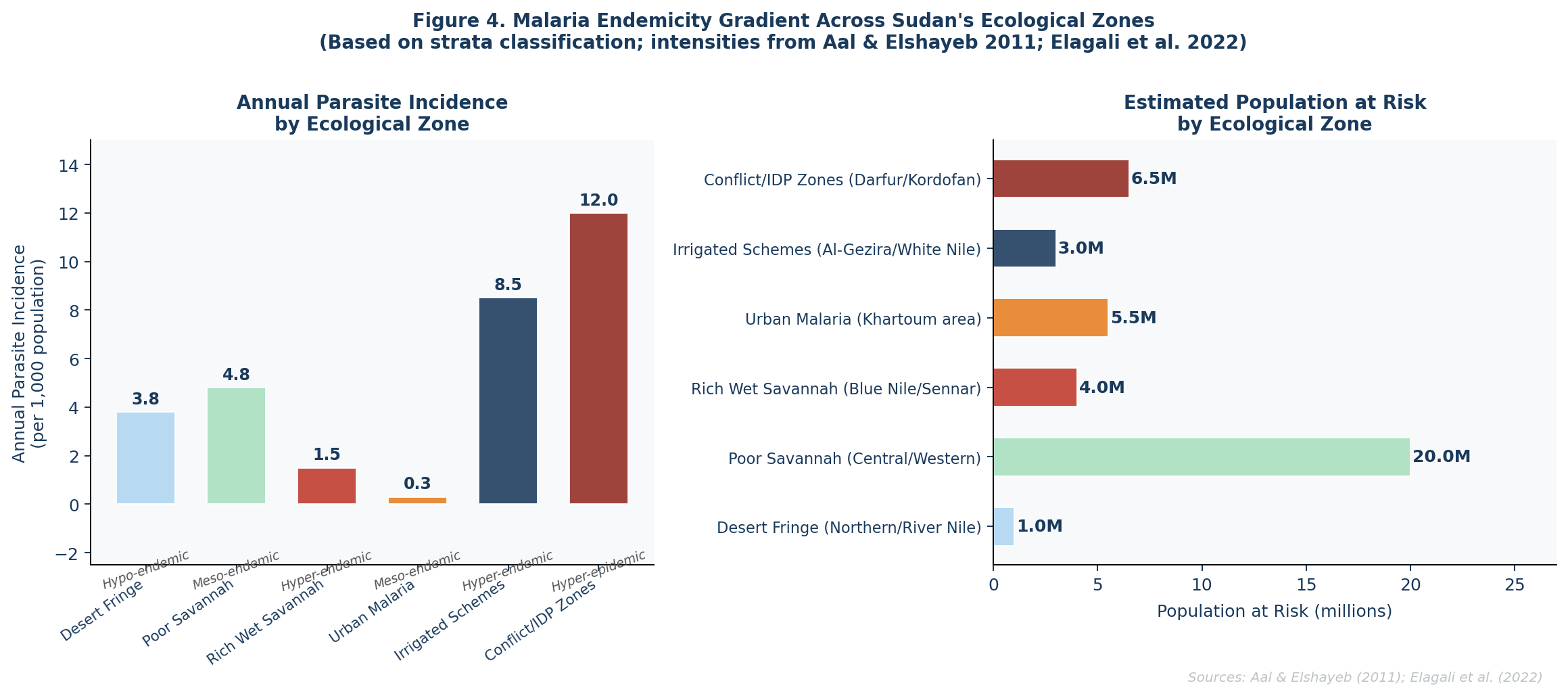
Sudan covers five principal ecological zones — ranging from the Sahara in the north to fertile savannah in the south — with a wide gradient of malaria transmission intensity, from hypoendemic on the desert edge to hyperendemic across central and southern states. Unlike many other human infectious diseases, seasonality remains a prominent characteristic of malaria epidemiology across the country, with transmission reaching peaks between October and December which follows-on from the rainy season spanning June to early November (Elagali et al., 2022).This seasonal rhythm has been repeatedly disrupted with extreme flooding events, particularly in 2018 and 2019, leading to massive population displacement, destruction of health infrastructure and ideal breeding conditions for mosquitoes.
In addition to climate, decades of war in Darfur, South Kordofan and Abyei have created millions of internally displaced persons (IDPs) huddled in camps with virtually non-existent health infrastructure. Indicators from the Ardamata IDP camp in West Darfur showed a malaria positivity rate of 61.1% by nested PCR — over five times higher than detected rates in better-resourced Khartoum-area camps (Eshag et al., 2020). These figures likely underestimate the true burden, as the access in health services in rural areas are estimated to be only at 20% (Aal & Elshayeb, 2011).
A second epidemiological change occurred with the 2019 discovery of the invasive vector Anopheles stephensi in Sudan — an urban-adapted mosquito that breeds in water containers, can withstand dry-season heat and has proven resistance to multiple classes of insecticides recommended by WHO, which threatens to expand malaria transmission into historically lower-risk urban settings (Elagali et al., 2022).
These pre-existing vulnerabilities have been catastrophically amplified since April 2023, when the outbreak of civil war between the Sudanese Armed Forces and the Rapid Support Forces triggered the world’s largest displacement crisis. By late 2024, over 10 million people had been internally displaced and an estimated 70–80% of health facilities in conflict-affected states had ceased functioning (WHO Sudan Situation Reports, 2023–2024). Malaria surveillance infrastructure — already fragile at 70% facility reporting completeness prior to the war — has largely collapsed in active conflict zones. The figures presented in this letter therefore represent a pre-war baseline; current burden is almost certainly substantially higher and must be urgently quantified once access permits.
1.2 Rationale and Objectives
This paper synthesises evidence from five key source documents to deliver a unified analytical framework covering disease burden, climate drivers, rural/IDP vulnerability, and cross-disease lessons from dengue control. The specific objectives are:
-
Characterise the malaria disease burden and spatiotemporal distribution across Sudan using national surveillance, Bayesian incidence mapping, and molecular epidemiology.
-
Analyse the statistical relationship between climatic factors - particularly rainfall and flooding - and malaria transmission dynamics.
-
Examine the specific epidemiological vulnerability of rural populations and IDP camps using molecular and survey data from conflict-affected areas.
-
To assess the applicability of dengue fever control principles to malaria in Sudan, develop evidence-based recommendations.
Patients identified from rural and remote populations in Sudan are disproportionately impeded from access to malaria prevention, diagnosis, and treatment services (only ~20% receive formal health care in rural areas). Such structural inequities drive delayed diagnosis, higher transmission and morbidity rates. Results: So, we show that to inform appropriate public health interventions, it is crucial to characterise transmission in rural and displacement settings.
Materials and Methods
2.1 Study Design
This study employs a structured narrative evidence synthesis methodology drawing on five primary source documents identified as directly relevant to the research objectives. Evidence synthesis was chosen over systematic review given the heterogeneity of study designs, settings, and data types across the sources, ranging from national surveillance-based Bayesian spatial models to cross-sectional molecular epidemiology studies and programme performance reviews.
2.2 Source Documents
Five documents were selected as primary data sources for this synthesis (Table 1). Data extraction covered: disease burden estimates (cases, deaths, positivity rates), epidemiological parameters (parasite species, vector data), climate correlations (statistical coefficients, lag times), intervention coverage and effectiveness, and qualitative programme findings.
| Reference / Source | Focus | Study Period | Setting / Sample |
| Elagali et al. (2022) - Scientific Reports | Spatiotemporal Bayesian malaria mapping in Sudan | 2017–2019 | Sudan national (n=461 facilities) |
| Aal & Elshayeb (2011) - AJEE | Climate change effects on malaria distribution | 1997–2007 | Sudan national (cross-sectional) |
| Eshag et al. (2020) - Trop Med & Health | Molecular epidemiology in Ardamata IDP camp | Jul–Dec 2018 | Al-Geneina City, W. Darfur (n=380) |
| Pasquale et al. (2013) - Malaria Journal | Malaria control in South Sudan 2006–2013 | 2006–2013 | South Sudan (national programme review) |
| Bridging Gaps in Dengue Management (2024) | Integrated public health response for dengue | 2024 (review) | Global (100+ countries) |
Sources were selected based on their relevance to rural health, climate-malaria relationships, and epidemiological burden in Sudan, with emphasis on studies addressing vulnerable and underserved populations.
Results
3.1 Disease Burden and Spatiotemporal Distribution
Flagging persistent, geographically heterogeneous malaria burden across of Sudan with evidence for both long-term endemicity and recent escalation. According to available historical government data, Sudan has an estimated 7–8 million cases of malaria each year and around 35,000 deaths annually from the disease with approximately 30–50% of outpatient visits due to malaria, as well as more than 20–30% hospital admissions (Aal & Elshayeb, 2011). In rural regions where health access is near 20%, these numbers both seriously underestimate the genuine burden.
The most up-to-date high-resolution data from the Bayesian spatiotemporal analysis (Elagali et al. 2022) suggest that the malaria burden in Sudan from 2015 to 2019 more than doubled. Sudan contributes 56% of all estimated malaria cases in EMRO — worsening despite regional declines elsewhere. At the species level, P. falciparum is dominant nationally (~87.6%), rising to 94.8% in IDP camps where P. vivax is comparatively rare (3.1%).
| Indicator | Data Value | Source | Notes |
| Malaria deaths/year (Sudan) | ~35,000 | Gov. records (Aal & Elshayeb, 2011) | Likely underestimate; rural access ~20% |
| Annual cases (Sudan) | 7–8 million | NMCP Health Centre records | 30–50% of outpatient visits |
| Cases doubled (Sudan, EMRO) | 2015–2019 | WHO data (Elagali et al., 2022) | Sudan contributes 56% of EMRO burden |
| Total cases 1997-2007 | 2,860,598 | NMCP (Aal & Elshayeb, 2011) | Annual mean: 87,411 cases |
| Malaria positivity - Ardamata IDP | 61.1% (232/380) | nPCR (Eshag et al., 2020) | P. falciparum only; males 67.1% |
| P. falciparum dominance | ~87.6% national | Sudan MIS 2016 (Elagali et al., 2022) | 94.8% in IDP camps |
| Peak malaria season | October-December | Routine surveillance (Elagali et al., 2022) | Follows rainy season (June–Nov) |
| South Sudan: malaria morbidity | 20-40% of all morbidity | HMIS (Pasquale et al., 2013) | Highest burden in sub-Saharan Africa |
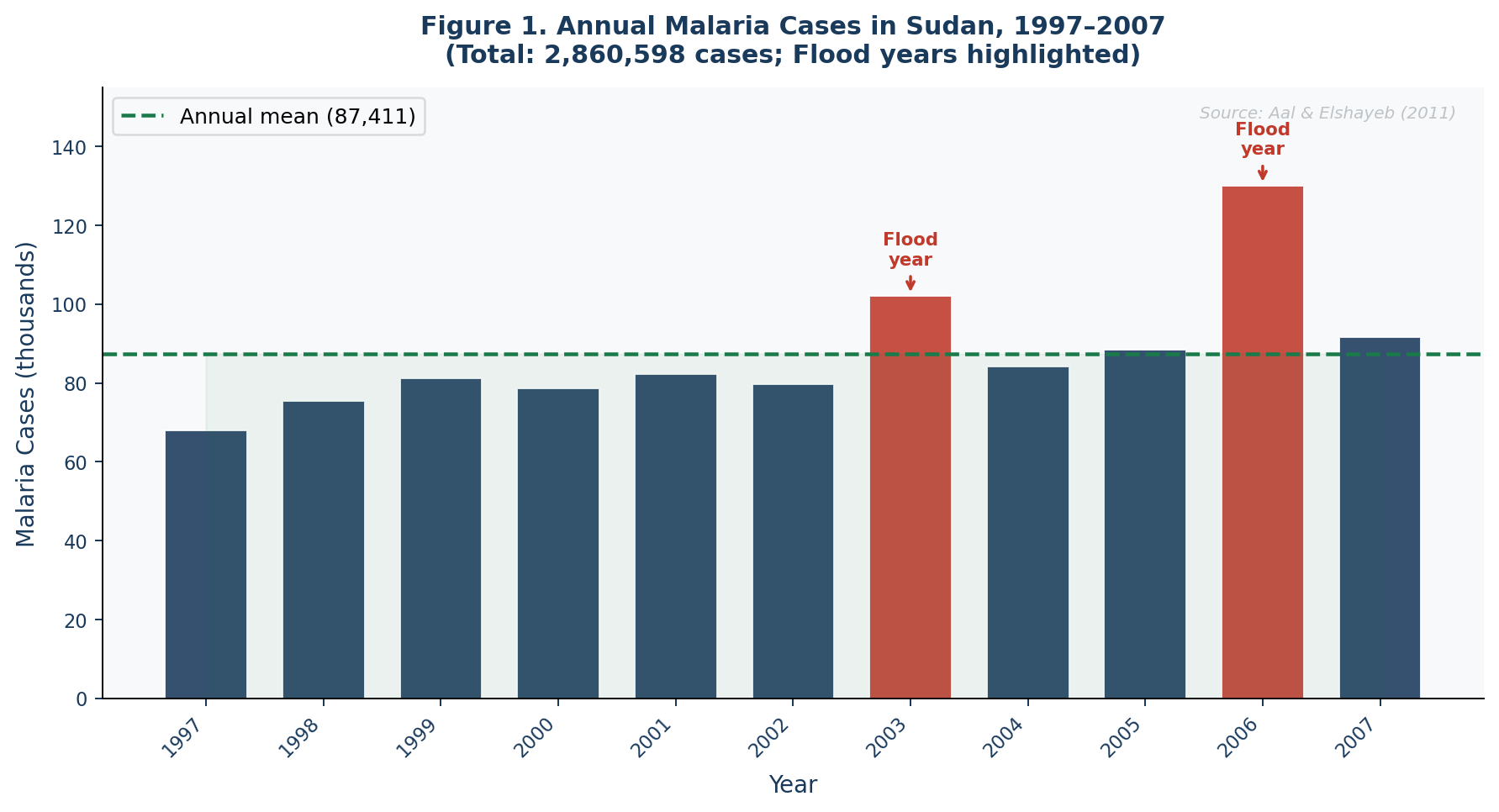
Figure 1 illustrates the fluctuating annual malaria case trend across 1997–2007, with marked peaks in 2003 and 2006 coinciding precisely with documented major flooding events. The linear trend (y = 190.96x + 68,007) showed a stable but persistent endemic pattern over the study period.
3.2 Rainfall, Flooding, and Malaria Transmission
Cross-correlation analysis (Aal & Elshayeb, 2011) showed significant positive associations between rainfall and malaria incidence (r>0.4, lag 1–3 months), temperature and relative humidity respectively (temperature r>0.5, lag 0–2 months; relative humidity r>0.5, lag 0). Mosquitoes have an aquatic development cycle that lasts 20 days at higher temperatures which shortens to 7 days, and more frequent blood feeding (high-risk). The most striking evidence of flooding as a causal force for malaria transmission stems from the extreme rainfall events of 2018-2019, where > 200,000 people across 15 states entered new areas at risk with declining health services simultaneously (Elagali et al., 2022).
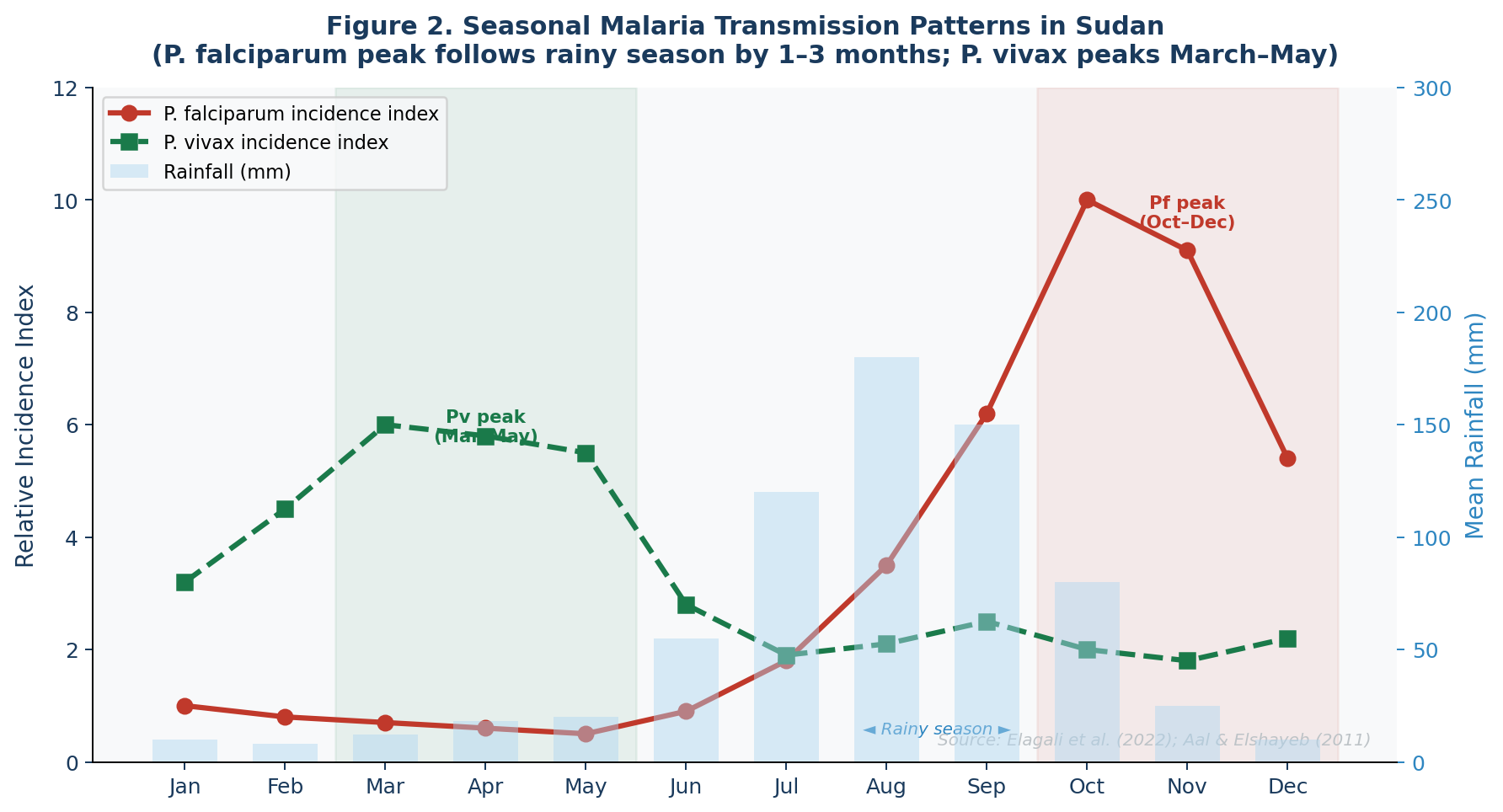
Figure 2 visualises the species-specific seasonal transmission patterns relative to the rainfall cycle. The 1–3 month lag between peak rainfall (July–September) and P. falciparum peak (October–December) creates a biologically predictable window for prospective early warning-based intervention deployment.
| Climate Variable | Direction | Lag / Timing | Evidence from Sources |
| Rainfall | Positive (r > 0.4) | Lag: 1–3 months | Strong correlation; flood events (2003,2006) caused highest malaria peaks |
| Temperature | Positive / complex | Lag: 0–2 months | Shortens mosquito aquatic cycle from 20 to 7 days |
| Relative Humidity | Positive (r > 0.5) | Lag: 0–2 months | Greatest relative impact (Spearman analysis) |
| Flooding events | Strongly positive | Immediate–3 months | 2018–2019 floods: 200,000+ displaced; increased breeding sites |
| Aridity | Negative (North) | Spatial | Hypoendemic in desert; hyperendemic in rich savannah |
| An. stephensi emergence | Urban risk amplifier | 2019 onward | Breeds in containers; resistant to IRS/ITN classes |
3.3 Rural and IDP Vulnerability
The evidence consistently indicates that Sudan's malaria burden is heavily concentrated in rural areas and displacement camps. The Ardamata IDP camp study (Eshag et al., 2020) found 61.1% malaria positivity by nested PCR among 380 suspected malaria patients — P. falciparum was the only species detected. This rate stands in stark contrast to the 5% and 11% positivity rates found in Khartoum-area camps where prevention activities are better maintained. Gender was the only statistically significant risk factor (COR = 1.55, p = 0.042), with males 1.5 times more likely to be infected due to occupational outdoor exposure.
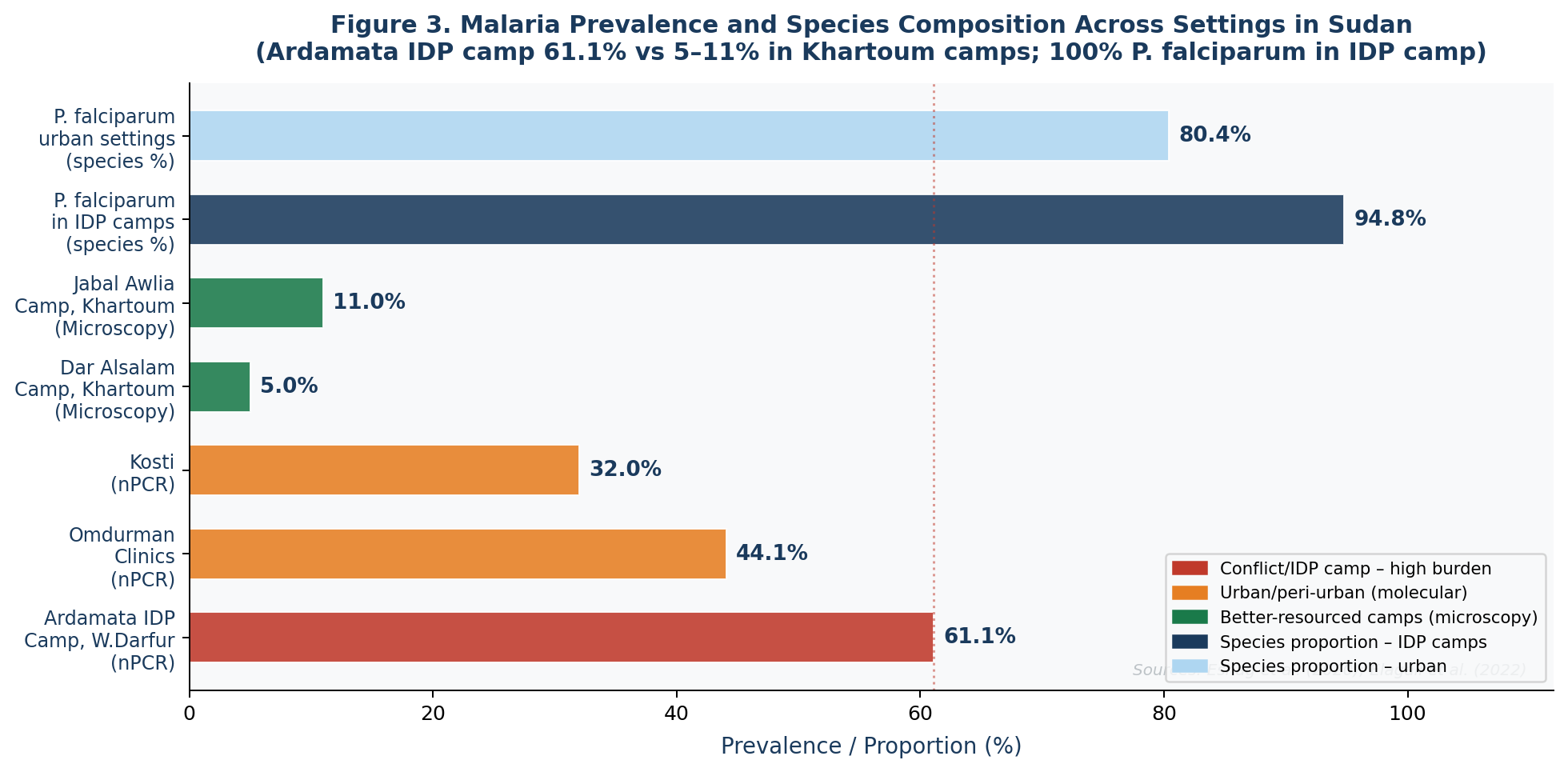
Figure 3 reveals the striking disparity in malaria burden across settings. The combination of high-sensitivity molecular diagnostics and conflict-driven vulnerability in the Ardamata camp produced positivity rates that are 5–12 times higher than in comparable urban settings, underscoring the urgent need for differentiated intervention strategies in IDP and rural contexts.
| Vulnerability Dimension | Sudan Data | South Sudan Data | Implication |
| Health service access | ~20% rural Sudan (Aal & Elshayeb, 2011) | 44% within 5 km (Pasquale et al., 2013) | Reduces early diagnosis; increases case fatality |
| Malaria positivity (IDP camp) | 61.1% nPCR – Ardamata (Eshag et al., 2020) | 5–11% microscopy – Khartoum camps | Molecular detection reveals true burden masked by surveillance |
| Dominant parasite (IDP) | P. falciparum 94.8% in IDP camps | P. falciparum >94% across South Sudan | Conflict-displaced face highest-virulence strain predominantly |
| Gender-based risk | Males 67.1% vs females 56.8% (p=0.042) | Occupational outdoor exposure – farming, fishing | Only significant risk factor in Ardamata camp study |
| Flood-displacement | 200,000+ displaced in 2018 floods | 131,990 conflict displacements (S. Sudan, 2013) | Displacement + flooding = compounded vulnerability |
| Reporting completeness | 70% overall (Sudan NMCP 2017–2019) | 68.8% reporting by Dec 2012 (South Sudan) | True burden substantially underestimated |
3.4 Intervention Coverage and Effectiveness
| Intervention | Approach | Documented Outcomes | Challenges |
| LLINs / ITNs | Mass campaigns + routine distribution | 9M+ nets in South Sudan; ownership 11.6%→53% (2006–2009) | Outdoor sleeping, net misuse, low coverage in conflict areas |
| IRS | Targeted; limited in conflict zones | Significant impact by Mentor Initiative (NGO, Malakal) | Resistance to DDT and deltamethrin detected |
| RDTs | Frontline PHC diagnosis | Confirmatory rate: 27% (2009) → 40% (2011) | HRP2/3 gene deletions cause false-negatives in Sudan |
| ACT | First-line treatment; artesunate+amodiaquine | Policy shift from CQ/SP after 40–93%/15–69% resistance | Stock-outs common; supply chain fragmented |
| IPTp | Through ANC services; SP-based | IPT2 uptake: 13%→58.2% (South Sudan) | SP resistance; late ANC attendance reduces coverage |
| Bayesian spatial mapping | 1×1 km incidence maps by species | Best-resolution malaria maps in EMRO | 70% facility completeness; sparse in remote areas |
| Integrated Vector Management | LLINs + IRS + larval source management | Adopted as main strategy post-CPA (South Sudan) | Financial/HR constraints prevent full IVM deployment |
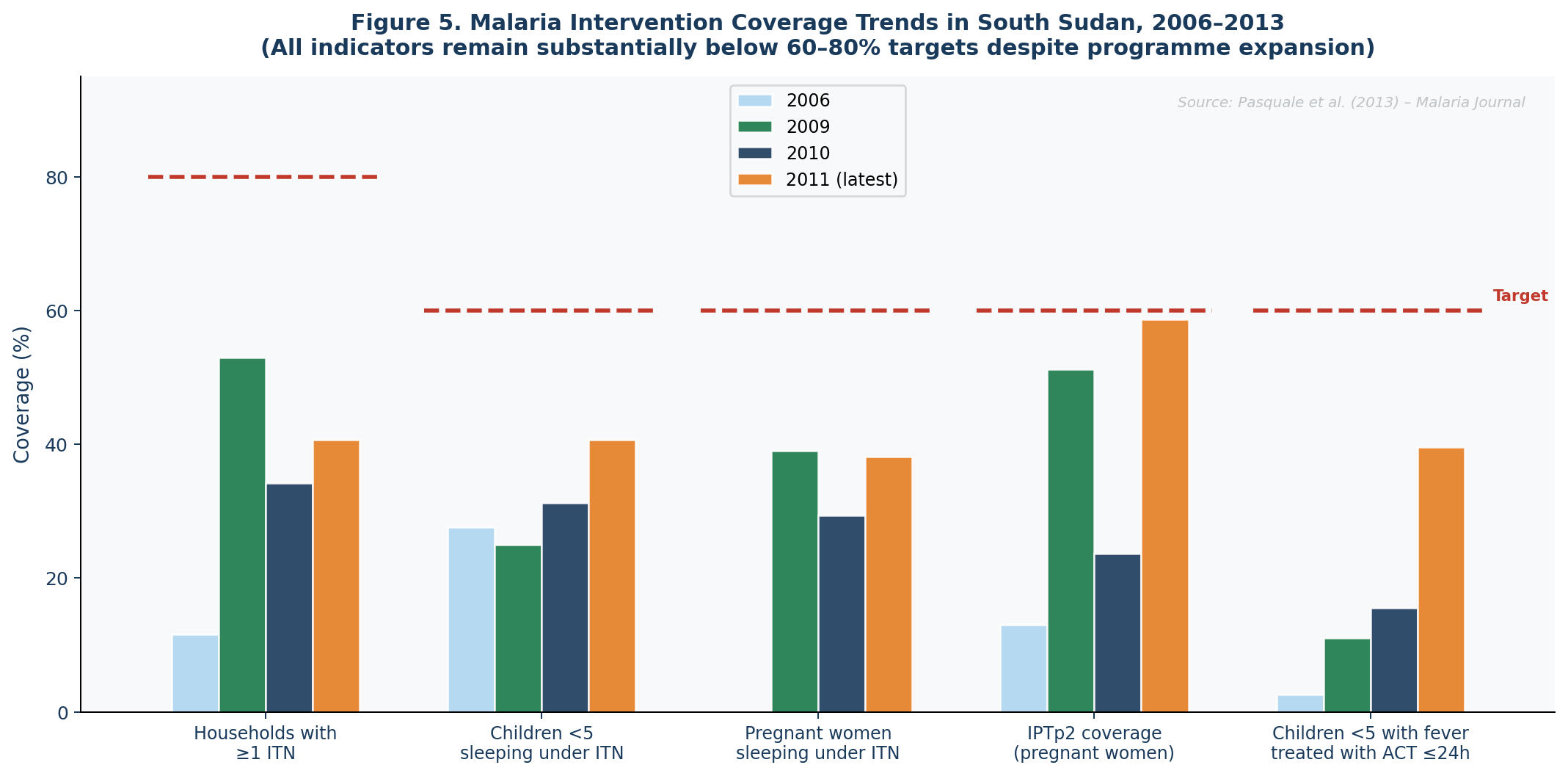
Figure 5 illustrates the persistent gap between achieved and target intervention coverage across South Sudan's malaria control programme. Despite 9 million LLINs distributed and substantial Global Fund investment (USD 170 million secured for 2008–2016), household ITN ownership peaked at 53% in 2009 against an 80% target, and child ACT treatment within 24 hours reached only 39.6% against a 60% target by 2011.
3.5 Lessons from Dengue Fever Control Applicable to Malaria in Sudan
The 2024 dengue management review synthesises transformative outcomes from integrated approaches: Wolbachia-based vector intervention achieved a 77% reduction in dengue cases and an 86% drop in hospitalisations, with a 45% spillover risk reduction in adjacent areas. AI-driven early warning systems improved outbreak prediction; the WHO COMBI framework demonstrated sustained vector breeding site reduction. Table 5 maps six dengue control pillars against their malaria control adaptations for Sudan.
| Dengue Pillar | Dengue Evidence | Malaria Adaptation (Sudan) | Feasibility |
| Integrated surveillance | Early warning through entomological + case monitoring | Climate-linked early warning integrating rainfall, flood, and monthly case data | Directly transferable; Sudan's 6-strata adds temporal dimension |
| Targeted vector control | Wolbachia: 77% case reduction; 86% hospitalisation drop | Larval source management (LSM) for An. stephensi container breeding | An. stephensi ecology directly analogous to Ae. aegypti |
| Diagnostic innovation | NS1, PCR, IgM/IgG, CRP, IPF% biomarkers | Molecular tools (nPCR) to overcome HRP2/3 deletion problem | nPCR not scalable; point-of-care equivalents needed |
| Community BCC | WHO COMBI framework; behaviour-informed interventions | Net use, fever reporting, stagnant water campaigns | Transferable; sustained community engagement essential |
| AI/data-driven early warning | AI outbreak prediction using climate + mobility data | ML models linking NMCP data + meteorological forecasts by state | Requires strong data infrastructure; 70% completeness a barrier |
| One-Health coordination | Human + veterinary + urban planning integration | Integration of NMCP with irrigation management and humanitarian response | Requires political commitment and multi-ministerial coordination |
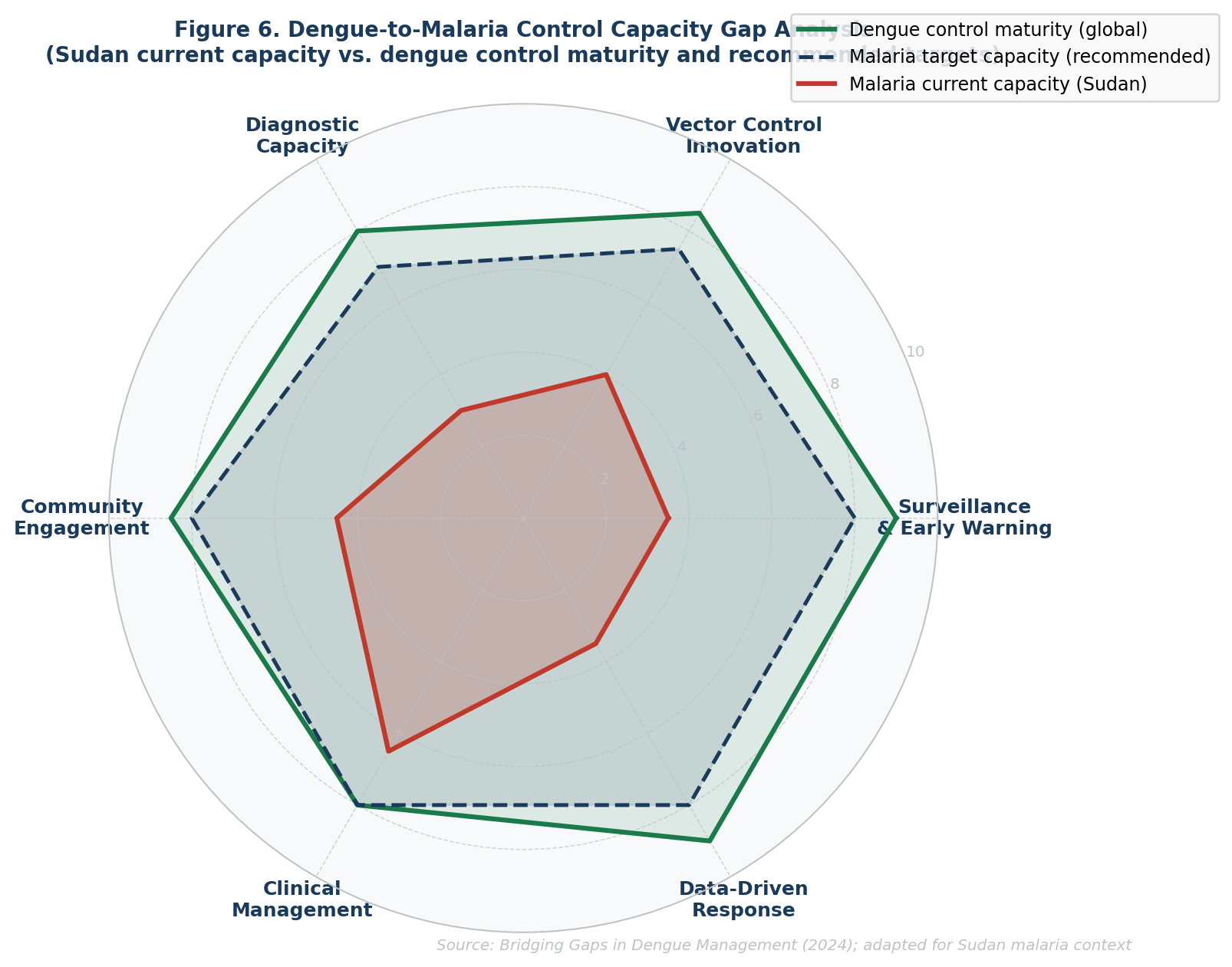
Figure 6 visualises the control capacity gap across six domains. The radar chart shows that Sudan's current malaria programme most closely approaches global standards in clinical management (treatment protocols), while the largest gaps remain in surveillance and early warning, AI/data-driven response, and diagnostic capacity — precisely the domains where dengue control has achieved the most transformative gains and where targeted investment would yield the greatest returns.
Discussion
4.1 Principal Findings
This study highlights that malaria in Sudan constitutes a deeply entrenched, climate-sensitive, and socially concentrated epidemic that cannot be controlled through any single intervention. Five interlocking conclusions emerge. First, the malaria burden is larger, more geographically heterogeneous, and more rapidly evolving than official statistics suggest. Second, rainfall and flooding are the most powerful environmental triggers of malaria transmission, operating through predictable biological lags that create windows for prospective intervention. Third, rural populations and IDP communities experience malaria intensities 5–12 times higher than urban settings with better health infrastructure. Fourth, the existing intervention portfolio remains inadequately scaled and poorly targeted. Fifth, dengue fever control offers a rich portfolio of transferable lessons if adapted appropriately.
4.2 Climate-Malaria Relationship: Implications for Early Warning
The consistent 1–3 month lag between rainfall and malaria incidence (Aal & Elshayeb, 2011) represents a prospective window not being systematically exploited. The Bayesian modelling framework of Elagali et al. (2022), which incorporated precipitation, aridity, and evapotranspiration as predictors at 1×1 km resolution, provides a ready-to-adapt technical blueprint for a national early warning system. A prospective system triggering pre-positioned resources before the malaria peak — rather than deploying in response to confirmed case surges — could substantially reduce morbidity and mortality, mirroring AI-driven dengue early warning architectures.
4.3 IDP and Rural Vulnerability: The Equity Dimension
The 61.1% malaria positivity rate in Ardamata IDP camp is not merely a statistic — it represents the human cost of compound vulnerability in conflict-displaced populations. Even where mosquito nets are nominally available (97.9% of Ardamata participants had nets), individual prevention is severely constrained by vector density, poor housing, outdoor occupational exposure, and inability to implement complementary indoor vector control. Intervention packages in IDP and rural settings must be substantially different from those in stable urban contexts. The dengue WHO COMBI framework — engaging communities as active participants rather than passive commodity recipients — offers a directly transferable model.
4.4 The HRP2/3 Diagnostic Challenge
The documented presence of pfrp2/3 gene deletions in Sudanese P. falciparum isolates (Elagali et al., 2022) causes false-negative HRP2-based RDT results — the frontline diagnostic tool at primary health care level across Sudan. This means that the already-limited confirmatory diagnosis rate (27–40%) includes a proportion of genuine P. falciparum infections systematically misclassified as negative. The cascade consequences include delayed treatment, ongoing transmission, and selection for drug-resistant parasite populations.
4.5 Applying Dengue Control Lessons: Opportunities and Constraints
Sudan's growing An. stephensi problem — a vector that, like Aedes aegypti, breeds in urban water containers — creates a specific context where container-targeting strategies from dengue control can be adapted with relatively minor modifications. However, the constraints on technology transfer must be acknowledged: Sudan's 70% facility reporting completeness introduces prediction uncertainty in areas with sparse coverage, and One-Health coordination faces substantial political barriers in a health system characterised by fragmentation. The dengue intervention toolkit offers methodology and systems architecture for transfer — not direct tool copying.
4.6 Implications for rural and remote health systems
This study found significant gaps in the delivery of health services in rural areas of Sudan. Restricted access to diagnostic services, delayed treatment and poor surveillance systems contribute to the perpetuation of malaria transmission in remote and conflict-affected areas. Rural settings, with an approximately 20% access share of the overall healthcare delivery system, demonstrate the need for decentralized service delivery models.
Investments are needed in stronger people-centered community health systems, with trained CHWs at their core, as well as mobile clinics and outreach diagnostic services. These approaches could also contribute to early detection or treatment, especially in remote or displacement (for example, refugee) settings.
Furthermore, integrating climate-relative early warning into rural health planning will provide a better lead time for the implementation of interventions ahead of peak transmissions. Such approaches are particularly relevant in those contexts where rainfall-driven dynamics of transmission can be foreseen.
Addressing malaria in these rural and remote populations requires a multi-pronged approach: biomedical interventions need to be combined with health systems strengthening, improved accessibility and community engagement linked to local realities.
Recommendations
Based on the synthesised evidence, the following ten priority recommendations are offered for Sudan's malaria prevention and control programme:
Recommendation 1: Establish a National Climate-Linked Malaria Early Warning System
Integrate NMCP monthly case data with Sudan Meteorological Authority rainfall and flood monitoring to generate 1–3 month lead-time malaria risk forecasts by state and locality. Build on the Bayesian spatiotemporal model of Elagali et al. (2022) as the analytical backbone and trigger pre-positioned resource deployment when rainfall exceeds historical norms in high-endemicity states.
Recommendation 2: Prioritise IDP and Rural Communities Post-Rainy Season
Allocate disproportionate intervention resources — ITNs, ACT, RDTs, mobile screening teams — to IDP camps and rural hotspots in the October–December peak transmission window. The Ardamata IDP camp data (61.1% positivity) demonstrates that standard coverage is insufficient; intensified, molecularly-guided strategies are required.
Recommendation 3: Conduct a National Survey of pfrp2/3 Gene Deletion Prevalence
Commission a country-wide assessment of HRP2/3 gene deletion frequency in P. falciparum isolates across Sudan's six ecological strata. Where deletion prevalence exceeds 5%, transition frontline RDT procurement to non-HRP2 tests to address the diagnostic accuracy gap currently undermining case detection.
Recommendation 4: Scale Up Integrated Vector Management in Irrigated Schemes
States with year-round malaria transmission (Al-Gezira, Sennar, White Nile) currently receive only single annual IRS rounds. Implement Larval Source Management (LSM) as an additional intervention layer and increase ITN coverage to the ≥80% threshold required for community-level protection.
Recommendation 5: Develop An. stephensi-Specific Urban Vector Control
Adapt container-elimination strategies from the dengue control playbook to target An. stephensi breeding sites in urban and peri-urban settings. Integrate with municipal water management authorities in Khartoum, Kassala, Red Sea, and Gedarif states where An. stephensi has been detected.
Recommendation 6: Implement Community BCC Following WHO COMBI Framework
Design state-specific behaviour change communication campaigns addressing outdoor sleeping, net misuse, and delayed care-seeking — with tailored messages for male outdoor workers, pregnant women, and IDP communities, following the dengue-proven COMBI methodology.
Recommendation 7: Strengthen Malaria in Pregnancy (MIP) Services
Implement three-dose IPTp in conjunction with free ITNs using existing ANC infrastructure Respond to persistently late ANC attendance through community health workers 1st contact service level, at household and camp.
Recommendation 8: Improve Health Facility Data Completeness
Invest in digital mHealth reporting tools to allow community health workers to submit their case data. Complement facility data with community-based passive surveillance to reduce the blind spots in high-burden rural areas with fewest facilities.
Recommendation 9: Establish Gender-Responsive Intervention Protocols
The significantly higher malaria positivity in males (COR = 1.55, p = 0.042) warrants targeted approaches for male occupational groups, including outdoor personal protection guidance (repellents, protective clothing) and male-specific BCC channels.
Recommendation 10: Integrate Malaria and Dengue Surveillance Infrastructure
Given Sudan now experiences both diseases, develop integrated vector-borne disease surveillance platforms sharing data infrastructure, laboratory capacity, and community reporter networks across malaria and dengue - reducing per-disease costs while creating synergistic early warning capacity.
Conclusion
Malaria in Sudan is not merely a health problem - it is a development emergency shaped by the intersection of climate variability, political instability, health system fragility, and deep geographic inequality. The evidence synthesised in this paper reveals an epidemic that is larger than official figures suggest, more concentrated among the most vulnerable populations, and more predictably linked to environmental triggers than current control programmes exploit.
The rainfall-malaria lag of 1–3 months creates a scientifically grounded opportunity for prospective, climate-driven intervention deployment. The 61.1% molecular malaria prevalence in the Ardamata IDP camp reveals the unacceptable human cost of inadequate protection in displacement settings. The close to doubling of cases between 2015 and 2019 in spite of sustained international investment indicates the need for a strategic step-change.
A view of control of dengue fever across the world provides both inspiration and a stepwise path to success. Wolbachia-based vector control, AI-driven early warning, community-centred behavioural approaches, and integrated public health architectures have collectively demonstrated that major sustained reductions in vector-borne disease burden are achievable even in resource-constrained settings. With careful adaptation to the biological realities of malaria and the social realities of Sudan, these lessons provide a credible evidence base for transforming Sudan's malaria control strategy.
Declarations
Ethics Statement
This study is a structured narrative review based exclusively on previously published literature and publicly available data sources. No human participants, identifiable patient information, or primary clinical data were directly involved; therefore, ethical approval and informed consent were not required.
Funding Statement
The author received no external funding for this study.
Conflict of Interest Statement
The author declares no conflict of interest.
Data Availability Statement
All data analyzed during this study are available from previously published sources cited within the manuscript.
AI Transparency Statement
Artificial intelligence-assisted technologies, including OpenAI ChatGPT, were used for language refinement, structural editing, formatting support, and manuscript organization. All scientific interpretation, literature evaluation, verification of content accuracy, and final manuscript approval were performed solely by the author, who assumes full responsibility for the integrity and accuracy of the work.