Introduction
Ocular morbidity describes eye diseases that are either significant to the individual or to the eye health professional. Visual impairment in childhood significantly affects the child’s development, education, and care given by families and professionals, and shapes the adult they become, influencing profoundly their employment and social prospects and opportunities throughout life. Visual impairment in the childhood if not detected early, affects the academic carrier of the child significantly. Thus although the prevalence and incidence of visual impairment are considerably lower in childhood than in adult life in all regions of the world, the relative burden, when considered in terms of years of life lived with visual impairment (person years of visual impairment) is considerable. Personal and social costs are important but difficult to measure. Significant childhood visual impairment leads to loss of economic productivity in the family[1].
“Vision 2020: The right to sight, a global initiative was launched by World Health Organization (WHO) and non-government organizations, for prevention of avoidable visual impairment, and children are the priority in this programme. For successful management of children with ophthalmic disorders, its early detection is most important [2]. WHO reports that there are approximately 19 million visually impaired children in the world, and 1.4 million are blind and three-quarters of these live in the poorest regions of Africa and Asia. About half of the causes of blindness and visual impairment are potentially preventable or treatable. Refractive error is an optical defect intrinsic to the eye which prevents the light from being brought to a single focus on the retina thus reducing normal vision. Refractive error, a major contributor to visual impairment, is a significant cause of morbidity among children worldwide. Undetected amblyopia, strabismus and significant refractive errors can have a significant long term effects on visual function and in some patients can cause permanent unilateral or bilateral vision loss. Childhood visual impairment due to refractive errors is one of the most common problems among school age children. Since children do not usually complain of visual difficulties, early detection and prompt treatment of eye is important to prevent visual problems and eye morbidities which could affect their learning ability, personality and adjustment in school. Ideally children should have repeated vision screening as they age since refractive errors and disruptions in binocular vision can develop at any age [3-5].
The spectrum of eye disease experienced by a population can be termed ‘ocular morbidity’. There is limited information about the prevalence of ocular morbidity in populations in developing countries. The ocular morbidity pattern, vary in different parts of the world and is influenced by racial, geographic, socio-economic and cultural factors. Five conditions: cataract, refractive errors/low vision, trachoma, onchocerciasis and vitamin-A deficiency and other causes of childhood blindness were determined to be responsible for 75% of all blindness worldwide. These are treatable and preventable [6-8].
Low vision is defined as a visual acuity (V/A) of less than 6/18, but equal to or better than 3/60, or a corresponding visual field loss of less than 20 degrees in the better eye with the best possible correction. On the other hand, blindness refers visual acuity of less than 3/60 or a corresponding field loss of less than ten degrees in the better eye with the best possible correction [9]. Knowledge of disease pattern in children can help design preventive and curative strategies. This study was conducted to determine the pattern of ocular morbidity among the primary school children in a block area.
Material &Methods
After taking permission from the Institutional ethical committee, a cross-sectional, school based survey was carried out among primary school children in the age group of 5 to 11 years. The study period was one year. All children studying in government and private primary schools, functional in one block area were included in the study. Children, whose parents/guardians/teachers did not give consent for detailed ocular examination were excluded from the study.
The Block Education Officer and the Principal/Headmasters of identified schools were informed about the study. They were also informed before each visit. All study subjects were examined as per pre-structured proforma after getting written informed consent from the teacher/guardian.
Ocular examinations was performed by one clinical team comprising, one data operator, one refractionists and two ophthalmologists. The study team had undergone one day intensive training for the staff for familiarization with the study protocol, equipment use, measurement methods, and data collection forms and data entry. The ocular examination was done in the schools. The examination included visual acuity (VA) assessment, ocular motility evaluation, examination of the external eye, anterior segment, media and fundus. The instruments and consumables used during the vision testing included: Snellen’s visual acuity chart (tumbling E), measuring tape (to measure 6 meters reading distance), trial lenses and frame, occluder, pinhole, pen torches with batteries, magnifying loupe, streak retinoscope, direct ophthalmoscope, cyclopentolate eye drops, and tobramycin eye drop. Cycloplegic and subjective refraction (For children with unaided VA 6/9 or worse in either eye) was done. Visual acuity testing was performed under normal daylight illumination using the Snellen’s tumbling E chart. This chart was placed on a wall six meters away from the child being examined. Each eye was evaluated separately, starting with the child’s right eye by covering the left eye; then the same procedure was repeated for the left eye by covering the right. Children being tested were instructed to use either hand (with their fingers extended) to show which direction the “fingers” of the E are pointing: right, left, up, or down. The examiners registered the smallest line which the child correctly read more than half the letters. In subjects with VA ≤ 6/12, a pinhole was presented and the test repeated. An improvement of the VA with pinhole was be considered refractive error. For those presenting with spectacles, VA was measured with their spectacles (presenting VA) and without spectacles (uncorrected VA). If the subject did not read even the first line of Snellen’s test types at a distance of six meters, he/she was asked to move one meter towards the chart till he/she was able to read the first line of the Snellen’s chart. If the subject still cannot read the chart from a distance of one meter, he/she was asked to count fingers at a distance of one meter and vision was recorded as ‘FC at one meter’. If subject cannot count fingers at one meter he/she was asked to count fingers at a distance of one foot and vision was recorded as ‘FC’ at one foot. Subject perceiving only hand movements close to face (HMCF) was recorded as ‘HMCF’. Subject with only perception of light (PL) was recorded as ‘PL +ve’ and projection of rays (PR) was tested in the four quadrants. It was recorded as ‘PR accurate’ or ‘PR inaccurate’. Subject who deny seeing any light with the full beam of a slit lamp bio-microscope of full intensity and no filters, was labeled as ‘PL negative’. Color vision was assessed using Ishihara color plates. Ocular motility was evaluated in all six cardinal positions of gaze and in nine diagnostic positions. Tropias were categorized as esotropia, exotropia, hypertropia and the degree of tropia measured using Hirschberg test. Binocular motor function was be assessed by ophthalmologists with a cover test at both 0.5 and 4.0 meters. Corneal light reflex was used to estimate the degree of deviation. The anterior segment (eyelid, conjunctiva, cornea, iris and pupil) and adnexa were examined by the ophthalmologist with a flashlight. Examination of the lens, vitreous and fundus was performed by the ophthalmologist using HEINE Beta A 200, direct ophthalmoscope inside a poorly lit part of the classroom in all the subjects. Children requiring further diagnostic tests or medical treatment were examined in a tertiary care centre.
Results
A total of 3650 children of 101 primary schools were studied. Of these schools 96 were Government primary schools and five were private primary schools. Of these 3650 students 2970 students were from government primary schools and 680 were from private schools. One thousand eight hundred and eighty students (51.5%) were male and 1770 (48.5%) were female. Five hundred and five (13.8%) children (277 male and 228 female) were detected to be suffering from some kind of ocular morbidity. Two hundred and seventy nine (279) children were found to have decreased visual acuity. Of these 272 were due to refractive error. Two each were suffering from optic atrophy, micro cornea and nystagmus respectively. One child had decreased V/A due to corneal opacity. The most common ocular morbidity was refractive error. The number of children with refractive error were 272 (7.5%). One hundred and thirty seven were male and 135 were female. Seventy two students (2%), were found to be suffering from color vision deficiency. Of these 66 were male and four were female. The color vision examination was done using Ishihara color plates. It was observed that, nine students were total color blind and 63 had red-green deficiency. Fifty eight students (Male:31,Female:27), were found to be suffering from allergic conjunctivitis (1.6%). Thirty seven students (1%), were found to suffering from some kind of ocular infections. Of these twenty nine students were suffering from blepharitis, five students had external hordeolum (stye), three students were suffering from acute conjunctivitis. Twenty four students (0.7%) were observed to be suffering from ocular motility disorders. Out of these six had alternate divergent squint, four had alternate convergent squint, five had exotropia, one had esotropia, six had exophoria, and two were suffering from horizontal nystagmus. Ten students had suffered from some kind of ocular trauma. Of these seven students had corneal opacity and one student had adherent leucoma and two students had injury scar marks over the eye lids. The other ocular morbidities were bluish discoloration of sclera (n=6), conjunctival nevus (n=4), chalazion (n=5), congenital ptosis (n=3), Xerophthalmia/Bitot spots (n=3), blue iris (n=3), trichiasis(n=2), madarosis (n=1), microcornea with iris coloboma (n=1). Ten children with special needs were also screened for ocular morbidity. They were suffering from mental retardation(n=5), deaf and mute(n=2), palate deformity(n=1), cleft lip(n=1), locomotor disability of lower limb(n=1). Out of these ten specially abled children, only one had ocular morbidity.
Discussion
Children comprise a major proportion of population and are important as they are the future of the country’s development. To study the pattern of ocular morbidity among children is important because while some eye conditions are just causes of ocular morbidity, others invariably lead to blindness. Childhood eye disorders can contributes significantly to the burden of blindness in a society when considered in terms of years of life lived with visual impairment. The majority of the causes of ocular morbidity are either preventable or treatable.
In this study of 3650(1880 male and 1770 female) primary school children aged between 5-11 years were studied. The prevalence of ocular morbidity was found in 505 (13.8%) primary school children (Table-1). Out of these 505 children with ocular morbidity, 276 were male and 227 were female. Nepal BP et.al.,[10]in their study reported that 11% (121 out of 1100) of the children in the age group of 5-16 years had ocular morbidity. Gupta M et.al.,[11] studied 1561 school children in the age group 6-16 years, and found 31.6% of ocular morbidity. The difference may be due to the age group and study area.
Two hundred and seventy nine children were found to have decreased visual acuity. Out of these,272 were suffering from refractive error (Table-1). Other causes of decreased vision were Optic atrophy (n=2), micro cornea (n= 2) and nystagmus (n=2). One child had decreased V/A due to central corneal opacity. Visual acuity testing was performed under normal daylight illumination using the Snellen’s tumbling E chart. Out of 7300 eyes of 3650 children, 6785 eyes (92.9%) had V/A of 6/6. Three hundred and seventy three eyes (5.1%) eyes had V/A in the range of<6/6 to 6/18. One hundred twenty five eyes (1.7%) had V/A in the range of <6/18 to 6/60. Fifteen eyes (0.2%) had V/A in the range of <6/60 to 3/60. One eye had V/A in the range of <3/60 to 1/60. This child was suffering from central adherent leucoma due to old trauma in the left eye which has V/A of 2/60. One eye had V/A in the range of <1/60 to PL positive. This child was suffering from traumatic optic atrophy in left eye and V/A in this eye was just PL positive. None of the eye was with PL negative (Table-2). The commonest cause of ocular morbidity in our study was refractive error with the prevalence of 7.5% (272 children) (Table-1). Out of these 272 children, 137 were male and 135 were female. Two hundred and forty three children were found to have myopia, 12 children were having astigmatism, ten children were suffering from hypermetropia and seven children were having hypermetropia associated with ocular motility defect (Figure-1). Only 19 children with the visual impairment were using glasses. Nepal BP et.al.,[10] in their study reported that 8.1%of the children in the age group of 5-16 years were suffering from refractive error and observed that the myopia was the most common refractive error. Rustagi et.al.,[12] studied 1075 school children in rural area of Delhi, in the age group of 11 to 18 years and reported 6.4%prevalence of refractive error. Both these studies are comparable to our study and the other India based studies (2.63-7.4%). Qian et.al.,[13] conducted ocular examination of 3248 students from primary and secondary schools in Tibet plateau which averages about 3500 m above the sea level. In their study the prevalence of myopia was 23.8% and that of hyperopia was 0.7%. Sewunetet.al.,[14] screened 432 primary school children in the age group of 6-15 years in Ehiopia and found overall prevalence of refractive error as 10.2% and myopia was the most common refractive error (5.47%). Previous studies have shown that the prevalence of myopia varies widely in various regions of the world. In western population myopia is found in one out of every three individuals. The difference may also be explained by different diagnostic criteria used by different authors, racial or ethnic variation in the prevalence of refractive error [11,13].
Seventy two students (1.97%), were found to be suffering from color vision deficiency. Of these 68 were male and four were female. The color vision examination was done using Ishihara color plates. It was observed that, nine students were total color blind and 63 had red-green deficiency. Defective red-green color vision affects 2-6% of the general population from a variety of defects that involve the color vision genes [15]. Since mostly color blindness is a genetic disorder, the incidence varies from race to race and across different geographical area. The common red/green color defects are sex-linked recessive traits and consequently men are primarily involved. Wale MJ et.al.,[16] reported prevalence of 4.2% color blindness among 850 primary school children in Ethiopia. The color vision testing should be done in the childhood to know the exact nature of defect, so that future of the child can be secured by choosing the right profession, eg if a person is having color vision defect, he is unsuited to be an engine driver or look-out man on a ship and he is unsuited to be a defense personnel.
Fifty eight students (1.6%), were found to be suffering from ocular allergies. Of these 31 were male and 27 were female (Table-1). There is a general paucity of data on prevalence of ocular allergies in general population worldwide. Many factors trigger allergic reaction like food, pollen etc. Spring time is the peak allergic season. Adequate recognition of ocular allergic conditions by children, parents, school and medical profession is needed. Preventive measures and prompt treatment of the symptoms should be recommended to the public and school administration. These included proper cleaning of the household, avoiding going to highly pollinated areas, more selective food etc[17].
Thirty seven students (1.0%), were found to suffering from some kind of ocular infections (Table-1). Of these twenty nine (0.8%) students were suffering from blepharitis, five students had external hordeolum or stye, three students were suffering from acute conjunctivitis. Most of the children (32 out of 37) suffering from ocular infections were from government primary school. Only five children with ocular infections were from private primary schools. In government primary schools the percentage of children suffering from ocular infections was 1.1% (32 out of 2970 children) while that in private primary schools was it was 0.7% (5 out of 680children). Blepharitis was present in 0.08% children in our study, while Singh V et.al.,[18] in their study in West Uttar Pradesh region of North India, reported 2.1 % prevalence of blepharitis among 4838 school going children in the age group of 5-15 years. Twenty four students (0.66%) were suffering from ocular motility disorders. Out of these 6 were suffering from alternate divergent squint (ADS), four had alternate convergent squint (ACS), 6 had Exophoria, five had Exotropia, one had Esotropia and two were suffering from horizontal nystagmus. Agrawal D et.al.,[19] studied prevalence of ocular morbidities among 1557 school children in the age group of 5-15 years and observed ocular motility disorders in 0.2 % children.
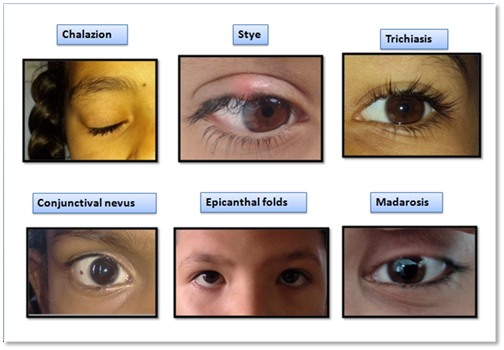
Ten students were having post trauma morbidities which includes, seven students with corneal opacity, one student with adherent leucoma and two students with injury scar marks over the eye lids (Figure-2).Other morbidities (Figure-3) which were less in number includes, bluish discoloration of sclera (n=6), conjunctival nevus (n=4), chalazion (n=5), congenital ptosis (n=3), Xerophthalmia/Bitot spots (n=3), blue iris (n=3), trichiasis (n=2), madarosis (n=1), micro cornea with iris coloboma (n=1).
In this study we screened ten children with special needs. Five students were mentally retarded, two were deaf and mute, one had palate deformity, one had cleft lip, one had locomotor disability of lower limb. Out of these ten children, seven were male and three were female. One child with mental retardation had alternate divergent squint (ADS) with refractive error in both eyes. In rest of the nine children with special needs the ocular examination was normal. Bhaskaran S et.al.,[20] in their study screened 243 children with special needs in seven schools, the mean age was 14.72. They found that the prevalence of refractive errors among children with special needs, was around 37% as opposed to the normal population, where it is 8%.
| S.NO. | Ocular Morbidity | Male | Female | Total (Percentage) |
| 1 | Refractive error | 137 | 135 | 272 (7.45%) |
| 2 | Color vision deficiency | 68 | 4 | 72 (1.97%) |
| 3 | Ocular allergies | 31 | 27 | 58 (1.59%) |
| 4 | Acute conjunctivitis | 0 | 3 | 3 (0.08%) |
| 5 | Xerophthamia | 2 | 1 | 3 (0.08%) |
| 6 | Conjunctival nevus | 1 | 3 | 4 (0.11%) |
| 7 | Scleral thinning (bluish discoloration) | 1 | 5 | 6(0.16%) |
| 8 | Corneal opacity | 3 | 4 | 7(0.19%) |
| 9 | Adherent leucoma | 0 | 1 | 1 (0.03%) |
| 10 | Micro cornea with iris coloboma | 0 | 1 | 1 (0.03%) |
| 11 | Iris nevus | 1 | 1 | 2 (0.05%) |
| 12 | Blue iris | 2 | 1 | 3 (0.08%) |
| 13 | Blepharitis | 15 | 14 | 29 (0.79%) |
| 14 | Ocular motility defects | 9 | 15 | 24 (0.66%) |
| 15 | Congenital ptosis | 2 | 1 | 3 (0.08) |
| 16 | Scar over eye lid | 0 | 2 | 2(0.05%) |
| 17 | External hordeolum | 1 | 4 | 5 (0.14%) |
| 18 | Chalazion | 1 | 4 | 5 (0.14%) |
| 19 | Trichiasis | 2 | 0 | 2 (0.05%) |
| 20 | Madarosis | 0 | 1 | 1 (0.03%) |
| 21 | Optic atrophy | 1 | 1 | 2 (0.05%) |
| Total | 277 | 228 | 505 (13.84%) |
| S.No | Visual acuity | Number of eyes |
| 1. | 6/6 | 6785 (92.94%) |
| 2 | <6/6 to 6/18 | 373 (5.11%) |
| 3 | <6/18 to 6/60 | 125 (1.71%) |
| 4 | <6/60 to 3/60 | 15 (0.21%) |
| 5 | <3/60 to 1/60 | 1 (0.03%) |
| 6 | <1/60 to PL positive | 1 (0.03%) |
| 7 | PL Negative | 0 |
| TOTAL | 7300 Eyes (100%) |


Conclusion
Primary school children being in the younger age group (5 to 11 years) are either afraid or are unable to express themselves due to which many diseases go unnoticed. Ocular examination including systemic examination should be made compulsory at the time of admission to primary schools. The children should be regularly examined medically thoroughly, and patiently, so that early detection can be done and longterm visual impairment reduced.
List of abbreviations
WHO-World Health Organization
VA-Visual Acuity
HMCF-Hand movements close to face
PL-Perception of light
PR-Projection of rays
Declarations
Ethics approval and consent to participate
Permission from Institutional Ethics Committee was taken vide Letter No.HFW-H-DR.DRKGMC/Ethics/2019/dated 27/02/2019.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
None
Funding Statement
Project was funded by Government of Himachal Pradesh.
Authors' contributions
Principal investigator: Dr Anil Kumar Verma
Co-Authors: Dr Anil Chauhan, Dr Shruti Anand
Acknowledgments
We acknowledge the contribution of Mr Pradeep Sharma, for providing services as refractionist for execution and completion of this project.