Introduction
Stroke is a major cause of mortality and long-term disability worldwide and represents a significant burden for patients, families, and healthcare systems. Global estimates indicate that approximately 15 to 16 million people experience a stroke each year, resulting in nearly 6 million deaths and leaving millions of survivors with permanent neurological impairments [1]. Stroke is currently the second leading cause of death and the leading cause of neurological disability globally [1,2].
Although substantial progress has been made in stroke prevention and management in high-income countries, outcomes remain poor in low- and middle-income countries, particularly in sub-Saharan Africa [2,3]. In these regions, the burden of stroke continues to increase due to population aging, urbanization, and the growing prevalence of cardiovascular risk factors [3]. Limited access to preventive care, delayed hospital presentation, and insufficient specialized stroke services further contribute to high mortality rates.
Stroke is broadly classified into ischemic and hemorrhagic subtypes. Globally, ischemic stroke accounts for nearly 80% of cases; however, hemorrhagic stroke is relatively more frequent in African populations [3,4]. This difference is largely explained by the high prevalence of uncontrolled arterial hypertension, which remains the most important modifiable risk factor for both ischemic and hemorrhagic stroke in Africa [5,6]. Hypertension is reported in more than 70–80% of African patients admitted for acute stroke [6].
The prognosis of stroke depends on multiple factors, including patient-related characteristics such as age and comorbidities, stroke-related factors such as type, location, and volume of brain injury, and the severity of neurological impairment at presentation [7,8]. In addition, the development of acute neurological or systemic complications—such as intracranial hypertension, seizures, infections, respiratory failure, and shock—plays a crucial role in determining outcomes [9-11].
Severe stroke often requires admission to an intensive care unit (ICU) for airway protection, invasive mechanical ventilation, hemodynamic support, management of intracranial hypertension, and close neurological monitoring [12,13]. In high-resource environments, the creation of specialized neurocritical care units and the accessibility of reperfusion therapies, such as intravenous thrombolysis and endovascular thrombectomy, have markedly enhanced survival and functional outcomes [14]. However, these advanced interventions remain largely unavailable in many African countries, where stroke management is predominantly supportive [12,15].
Several studies conducted in sub-Saharan Africa have reported high mortality rates among stroke patients admitted to ICUs, frequently exceeding 40–60% [15-17]. The Democratic Republic of the Congo (DRC) has limited data on stroke outcomes in intensive care settings. Mukeng et al. reported that stroke accounted for approximately 11.7% of ICU admissions in Lubumbashi, with a predominance of hemorrhagic stroke [18]. Tshituta et al. highlighted the high frequency of metabolic disturbances, particularly hyperglycemia, during the acute phase of stroke and their association with poor outcomes [19].
Despite these findings, there is a lack of multicenter studies describing clinical phenotypes, complications, and survival patterns of stroke patients admitted to ICUs in Kinshasa. A deeper understanding of these factors is essential for improving early risk stratification, optimizing management strategies, and guiding the allocation of limited healthcare resources.
Therefore, this multicenter study aimed to describe the clinical phenotypes and survival of patients admitted for acute stroke to intensive care units in Kinshasa and to identify factors associated with in-hospital mortality.
Methods
2.1. Study Design
This study was a multicenter cross-sectional investigation conducted to describe the clinical phenotypes and survival of patients admitted for acute stroke to intensive care units (ICUs) in Kinshasa, Democratic Republic of the Congo. The primary aim was to provide a detailed description of patient characteristics, complications, and outcomes during ICU admission.
2.2. Setting
The study took place in the ICUs of four tertiary hospitals in Kinshasa. Data collection was performed over a four-month period, from July 1 to November 1, 2023. These hospitals provide critical care services for a broad range of patients, including those with severe neurological conditions. The ICUs included general and neurology-specific beds and were equipped with imaging facilities and standard life-support interventions. Advanced reperfusion therapies were not routinely available in these settings.
2.3. Participants
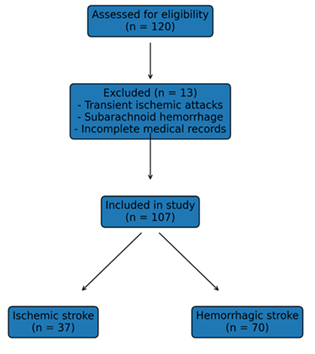
All adult patients (≥18 years) admitted to the participating ICUs for acute ischemic or hemorrhagic stroke were eligible. Stroke diagnosis was confirmed by brain imaging (computed tomography or magnetic resonance imaging). Patients with transient ischemic attacks, subarachnoid hemorrhage, or incomplete medical records were excluded. Consecutive admissions that met the inclusion criteria during the study period were enrolled. No additional matching or selection procedures were applied, consistent with a cross-sectional study design.
2.4. Variables
The primary outcome was in-hospital mortality. Secondary outcomes included length of ICU stay and the occurrence of neurological or systemic complications. Predictor variables included demographic characteristics (age, sex), clinical features (blood pressure, Glasgow Coma Scale, neurological signs), comorbidities (hypertension, diabetes, cardiovascular disease), laboratory findings (blood glucose, renal function), radiological characteristics (stroke type and location), and therapeutic interventions (mechanical ventilation, vasopressors, osmotherapy). Potential confounders such as age, comorbidities, and stroke severity were identified in advance.
2.5. Data Sources and Measurement
Data were extracted from medical charts and ICU records using a standardized case report form. Clinical assessments, laboratory tests, and imaging interpretations followed hospital protocols. All participating sites used comparable methods, including standardized neurological scales and laboratory quality control procedures, to ensure uniformity across centers.
2.6. Bias
To minimize bias, consecutive patient enrollment was applied to reduce selection bias, and standardized data extraction forms were used to limit information bias. All data were cross-checked by two independent investigators to ensure completeness and accuracy.
2.7. Study Size
The study included all eligible patients admitted during the four-month study period. Based on prior ICU admission rates and stroke prevalence in Kinshasa, this sample was expected to provide adequate representation of the ICU stroke population.
2.8. Quantitative Variables
Continuous variables such as age, blood pressure, and laboratory values were summarized using means ± standard deviations or medians with interquartile ranges, depending on distribution. Categorical variables, including stroke type and presence of complications, were presented as counts and percentages. For some continuous variables, such as the Glasgow Coma Scale, clinically relevant cutoffs were used for categorization.
2.9. Statistical Methods
Data were entered into a secure database and analyzed using standard statistical software. Descriptive statistics were applied to summarize patient demographics, clinical characteristics, complications, and outcomes. Comparisons between survivors and non-survivors were performed using chi-square or Fisher’s exact tests for categorical variables and t-tests or Mann–Whitney U tests for continuous variables, as appropriate. To deal with missing data, the number of available observations for each variable was reported, and sensitivity analyses were done to see how missing values affected the results. All analyses were descriptive and aimed at characterizing the ICU stroke population. Statistical significance was not the primary focus, as the study was descriptive in nature.
Results
3.1. Participants
During the study period (July 1 to November 1, 2023), a total of 107 adult patients were admitted to the ICUs of four tertiary hospitals in Kinshasa for acute stroke. Stroke was confirmed by brain imaging for all patients. Among them, 37 patients (34.6%) were diagnosed with ischemic stroke, while 70 patients (65.4%) had hemorrhagic stroke. The flow of study participants is summarized in Figure 1.
3.2. Demographic characteristics
Table 1 presents the demographic characteristics of patients according to stroke type. Overall, patients were predominantly male, with 61% of the cohort being men. The mean age was 61.7 years, ranging from 26 to 89 years, with patients older than 55 years being the most represented. Most patients were married (83%).
When examining the groups separately, the male predominance was observed in both ischemic and hemorrhagic strokes, with 54% and 64% respectively. Patients with hemorrhagic stroke tended to be slightly older (mean age 63.3 years) compared to ischemic stroke (mean age 59.2 years), although this difference was not statistically significant. Age distribution and marital status were similar across stroke types (Table 1).
| Variable | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Male sex, n (%) | 20 (54%) | 45 (64%) |
| Female sex, n (%) | 17 (46%) | 25 (36%) |
| Mean age, years (range) | 59.2 (26–85) | 63.3 (28–89) |
| Age ≥60 years, n (%) | 21 (57%) | 49 (70%) |
| Married, n (%) | 31 (84%) | 58 (83%) |
3.3. Comorbidities
Comorbidities were frequent in this ICU stroke population. Hypertension was the most common comorbidity, affecting 76–77% of patients in both stroke groups. Diabetes and obesity were also frequently observed, present in around one-quarter of patients. Other comorbidities, including previous stroke, cardiovascular disease, nephropathy, smoking, and alcohol use, were less common (Table 2).
There was no statistically significant difference between ischemic and hemorrhagic stroke groups in terms of comorbidities. Overall, the profile of comorbidities highlights the high cardiovascular risk burden in this population.
| Comorbidity | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Hypertension | 28 (76%) | 54 (77%) |
| Diabetes | 10 (27%) | 16 (23%) |
| Obesity | 8 (22%) | 16 (23%) |
| Cardiovascular disease | 3 (8%) | 3 (4%) |
| History of stroke | 7 (19%) | 13 (19%) |
| Nephropathy | 1 (3%) | 5 (7%) |
| Smoking | 6 (16%) | 17 (24%) |
| Alcohol | 3 (8%) | 5 (7%) |
3.4. Clinical presentation at ICU admission
Table 3 summarizes the main reasons for ICU admission and clinical presentation. Altered consciousness was the most frequent presenting feature, observed in 80 patients (75%). Hemorrhagic stroke patients more commonly presented with altered consciousness (89%) compared to ischemic stroke patients (65%). 42% of the total population had major motor deficits, and the same percentage was true for each type of stroke. Other less frequent features included dysarthria, convulsions, acute respiratory distress, and sensory-motor deficits. Sensory-motor deficits were more frequently observed in ischemic stroke patients (24%) than in hemorrhagic stroke patients (3%).
| Variable | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Altered consciousness | 24 (65%) | 62 (89%) |
| Major motor deficit | 15 (41%) | 30 (43%) |
| Dysarthria | 1 (3%) | 1 (1%) |
| Acute respiratory distress | 2 (5%) | 6 (9%) |
| Sensory-motor deficit | 9 (24%) | 2 (3%) |
These findings underline that patients with hemorrhagic stroke were more likely to present with a depressed level of consciousness, while ischemic stroke patients more frequently had sensory-motor deficits.
3.5. Physical examination
At ICU admission, 98% of patients had an altered general state. A Glasgow Coma Scale (GCS) score of ≤8 was observed in 40% of patients overall, with a much higher proportion in hemorrhagic stroke (57%), compared to ischemic stroke (18%). Hemiplegia (59%) and facial paralysis (27%) were the main focal neurological signs. Cardiac and pulmonary examinations were normal in the majority, with only 26% and 16% showing abnormalities, respectively. Hydration and deep tendon reflexes were altered in 22% and 12% of patients, respectively (Tables 4).
| Variable | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Glasgow ≤8 | 8 (18%) | 40 (57%) |
| Mydriasis | 3 (8%) | 17 (24%) |
| Myosis | 5 (14%) | 18 (26%) |
| Hemiplegia | 22 (59%) | 41 (59%) |
| Facial paralysis | 10 (27%) | 19 (27%) |
3.6. Laboratory and imaging findings
Laboratory assessments were performed in all patients. Most biological parameters were comparable across stroke types, except for serum sodium, which was significantly higher in hemorrhagic stroke (154 mmol/L) compared to ischemic stroke (139.5 mmol/L). Brain imaging confirmed the diagnosis in all patients, with 97% of scans performed within 48 hours. Hemorrhagic strokes represented 65% and ischemic strokes 35% of the total (Table 5).
| Variable | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Sodium (mean mmol/L) | 139.5 | 154 |
| Brain imaging within 48h | 36 (97%) | 68 (97%) |
3.7. Therapeutic interventions
All patients received general supportive care. Specific interventions varied by stroke type. Mannitol and vasopressors were more frequently used in hemorrhagic stroke, and mechanical ventilation was required in 48% of patients, predominantly in hemorrhagic strokes. Surgical procedures, including tracheostomy and other neurosurgical interventions, were performed when indicated (Table 6).
| Intervention | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Oxygen therapy | 35 (95%) | 64 (91%) |
| Mannitol | 12 (32%) | 39 (56%) |
| Antibiotics | 16 (43%) | 48 (69%) |
| Mechanical ventilation | 16 (43%) | 38 (54%) |
| Tracheostomy | 3 (8%) | 10 (14%) |
3.8. Complications
During the ICU stay, complications were common. Pneumonia (39%), non-pulmonary infections (22%), and shock (21%) were the most frequent. Hemorrhagic stroke patients experienced a higher rate of complications than ischemic stroke patients (Table 7).
| Complication | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Shock | 3 (8%) | 19 (27%) |
| Intracranial hypertension | 0 | 7 (10%) |
| Pneumonia | 8 (22%) | 34 (49%) |
| Seizures | 7 (19%) | 18 (26%) |
| Acute kidney injury | 3 (8%) | 12 (17%) |
| Infection | 4 (11%) | 19 (27%) |
3.9. ICU outcome
Overall ICU mortality was 58% (62 patients), with higher mortality in hemorrhagic stroke (44 patients, 63%) compared to ischemic stroke (18 patients, 49%) (Table 8).
| Outcome | Ischemic stroke n=37 | Hemorrhagic stroke n=70 |
| Death | 18 (49%) | 44 (63%) |
| Survival | 19 (51%) | 26 (37%) |
Patients with hemorrhagic strokes had a higher risk of death during ICU stays, reflecting the severity of this stroke type.
Discussion
This multicenter study provides important insights into the clinical phenotypes and survival of stroke patients admitted to intensive care units in Kinshasa. The results indicate that hemorrhagic stroke was the predominant subtype among ICU admissions, that patients frequently presented with severe neurological impairment, and that in-hospital mortality was high, particularly among those with hemorrhagic stroke. These findings directly address the study objective of describing stroke severity, complications, and outcomes in a critical care context in a low-resource setting.
The predominance of hemorrhagic stroke observed in this cohort contrasts with global epidemiological data, where ischemic stroke accounts for approximately 80% of cases [1], but is consistent with numerous studies conducted in sub-Saharan Africa [3,5,6,15-18]. The high prevalence of uncontrolled arterial hypertension, affecting more than three-quarters of patients in both stroke subtypes, largely explains this pattern. Hypertension has been consistently identified as the most important modifiable risk factor for both ischemic and hemorrhagic stroke in African populations [5,6], and its poor detection and control remain a major public health challenge in the region [3,18]. The relatively younger age of patients compared with cohorts from high-income countries further reflects earlier exposure to cardiovascular risk factors and limited access to preventive care.
Stroke severity at ICU admission was marked, particularly among patients with hemorrhagic stroke, who more frequently presented with altered consciousness, low Glasgow Coma Scale scores, and pupillary abnormalities. These clinical features are well-established predictors of poor outcome in acute stroke [8,13] and explain the higher need for mechanical ventilation, osmotherapy, and vasopressor support observed in this group. The predominance of focal sensory-motor deficits among ischemic stroke patients is consistent with classical ischemic stroke presentations described in the literature [7], whereas depressed consciousness and signs of intracranial hypertension are more typical of severe hemorrhagic stroke [4,12].
Complications during ICU stay were common and played a central role in patient outcomes. Infectious complications, particularly pneumonia, were the most frequent, affecting nearly two-fifths of patients. This finding is in line with previous studies showing that post-stroke infections are among the most common and lethal complications in critically ill stroke patients [9-11]. Pneumonia, in particular, has been shown to significantly increase mortality, prolong ICU stay, and worsen neurological outcomes [10,11]. The higher frequency of shock, acute kidney injury, and seizures among hemorrhagic stroke patients likely reflects greater initial severity, prolonged mechanical ventilation, and systemic physiological stress, all of which have been associated with poor prognosis in ICU-admitted stroke patients [12,13].
The overall ICU mortality rate of 58% observed in this study is high but comparable to rates reported in other African intensive care settings, including studies from Djibouti, Brazzaville, and Dakar, where mortality among severe stroke patients frequently exceeds 40–60% [15-17]. In contrast, mortality rates reported in high-income countries are substantially lower, reflecting differences in stroke systems of care, earlier hospital presentation, availability of specialized neurocritical care units, and access to reperfusion therapies [12-14]. The absence of intravenous thrombolysis and endovascular thrombectomy in the study settings likely contributed to poor outcomes, particularly among ischemic stroke patients who might otherwise benefit from timely reperfusion [14,20].
Several limitations should be considered when interpreting these findings. The cross-sectional design does not allow causal inference or identification of independent predictors of mortality. The relatively short study period and modest sample size may limit statistical precision and the ability to explore interactions between clinical variables. Selection bias is likely, as the study included only patients admitted to ICUs, representing the most severe end of the stroke spectrum and potentially overestimating mortality compared with the general stroke population. Information bias related to retrospective data extraction from medical records is also possible, although standardized data collection and cross-checking were used to minimize this risk. In addition, important variables such as stroke volume, standardized stroke severity scores, and long-term functional outcomes were not available, which may have resulted in residual confounding.
Despite these limitations, the consistency of the findings with previous studies from similar settings supports their validity. The results highlight the combined impact of severe initial neurological injury, high burden of comorbidities, frequent complications, and limited access to advanced therapies on stroke outcomes in low-resource ICUs. From a public health perspective, these findings point to the urgent need for improved primary prevention, particularly better detection and control of hypertension, as well as strengthening of early stroke care and basic neurocritical care practices, including airway protection, infection prevention, and hemodynamic monitoring.
The generalizability of these results should be interpreted with caution. As the study was conducted in tertiary hospitals in an urban setting and focused exclusively on ICU-admitted patients, the findings may not apply to patients with milder stroke or those managed in non-specialized facilities. However, given the similarities in healthcare infrastructure, resource constraints, and cardiovascular risk profiles across many urban centers in sub-Saharan Africa, these results are likely relevant to comparable low- and middle-income settings. This study therefore provides valuable evidence to inform clinical practice, resource allocation, and future research aimed at improving outcomes for critically ill stroke patients in Africa.
Conclusion
This multicenter study demonstrates that critically ill stroke patients admitted to ICUs in Kinshasa present predominantly with hemorrhagic stroke, severe neurological impairment, and a high burden of comorbidities, particularly hypertension. Complications during ICU stay are frequent and significantly contribute to poor outcomes, resulting in an overall in-hospital mortality of 58%, with higher mortality among hemorrhagic stroke patients. These findings point to the need for improved primary prevention, early recognition, and optimized critical care management in low-resource settings. Strengthening hypertension control, early stroke care pathways, and basic neurocritical care practices may help reduce mortality and improve outcomes for this high-risk population.
Declarations
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Author Contributions
Rodrigue Ngwizani, Arriel Makembi Bunkete, Kazi Anga Muamba: Conceptualization, study design, data collection, and manuscript drafting.
Eric Amisi, Lays Kukamba, Tharcisse Mabiala, Patrick Mukuna, Wilfrid Mbombo, Medard Bulabula, Berthe Barhayiga: Data collection, patient management, and critical revision of the manuscript.
All authors: Approved the final manuscript and agree to be accountable for all aspects of the work.
Acknowledgements
The authors would like to thank the staff of the ICUs of the University Clinics of Kinshasa for their collaboration and support during data collection, as well as all patients and their families for their participation.
Ethical Considerations
The research protocol was approved by the Scientific Committee of the Department of Anesthesia-Resuscitation of the University Clinics of Kinshasa (CUK) and subsequently by the Ethics Committee of the University of Kinshasa (Approval Number : ESP/CE/116/2023). All procedures were conducted in accordance with the Declaration of Helsinki, respecting confidentiality and ethical standards. Written informed consent was obtained from patients or their legally authorized representatives prior to inclusion.
Consent to Publish
All authors have reviewed and approved the manuscript and consent to its publication in the journal.
Availability of Data and Materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.